

Steve Parker, Editor in Chief of The Profitable Dentist Magazine along with Paula Parker, TPD Director of Business Operations, recently sat down with Dr. Tom Nabors to discuss his pioneering efforts and ongoing research and expertise around saliva testing.
Steve:
Today, we are interviewing Dr. Thomas Nabors.
Dr. Nabors is often referred to as the “Father of Saliva Testing.”. Tom and his son, Dr. Tommy Nabors, are the original pioneers in bringing saliva testing into the U.S. beginning way back in 2001. He has over 40 years of both clinical and scientific research: Plus, over 40,000 case studies supporting saliva testing. Along with introducing this DNA technology as a medical grade diagnosis, Tom has revolutionized the bridge between periodontal diseases and systemic medicine in the truest sense.
Dr. Nabors, welcome to this unique discussion. Let me start by asking, how did you get started down this path and why do we need saliva testing for periodontal disease?
Dr. Tom Nabors:
First, thank you, Steve and Paula, for asking me to be a part of this important conversation.
Let me begin by stating this … saliva testing for very specific markers of disease has truly moved periodontal medicine into the 21st century. It is the first real paradigm shift in thinking and in technology in periodontal care in the past 130 years.
Simply put, using DNA technology from a 1ml of saliva sample connects this infectious inflammatory disease that we call “periodontal disease” to objective causative events rather than subjective observation.
For many years, I was frustrated with the “classification” system and the unpredictability of the traditional treatment model. So, these two things have driven me to commit most of my life to improving our diagnosis, our treatment objectives, treatment outcomes, and a scientific method of connecting these infections to the rest of the body.
Paula:
This sounds like a revolutionary approach.
Dr. Tom Nabors:
Think about this for a minute … dentists, dental hygienists and periodontists are taught that a periodontal probe, which was invented in 1936, is the most sophisticated technological instrument in periodontal disease history.
If the entire world of dentistry had not progressed in technology in all other areas of oral health beyond 1936, where would we be? There would be no cosmetic dentistry, no implants, no airway discoveries, no TMJ therapy, no endodontics, etc. We would still be tooth-pullers and denturists.
Steve:
That is an interesting thought. Do you have evidence that saliva testing is supported by current literature reviews?
Dr. Tom Nabors:
Yes, large volumes of oral microbiology, immunology, medical research, and periodontal clinical trials confirm that the periodontal probe is not a diagnostic instrument, and that we are treating periodontal infections as if all infections are the same.
And, of course, these infections are very different, and we must first understand their differences.
In fact, much of the literature of today, more specifically the medical literature, is demanding that we move into saliva testing and this world of DNA technology. Personalized diagnosis and treatment improve both periodontal diseases as well as diseases caused by systemic inflammation.
Paula:
In simple terms, how should a dentist or a hygienist think relative to saliva testing’s purpose?
Dr. Tom Nabors:
The clinician should think of a saliva test in the same way that one thinks of a CBCT scan. We all know how this technology has dramatically improved our diagnosis and treatment models.
Relative to a CBCT and this comparison to a saliva test, the same principles are true. A saliva test provides critical information that we cannot see or measure clinically.
Saliva testing provides objective information connecting …
- Accurate “targets of therapy” (biofilm is too generalized)
- Disease severity based upon the infection species and the medical history rather than pocketing (what’s causing dysbiosis and disease?)
- Personalized treatment (reducing or eliminating the real targets of therapy)
Steve:
So, what can we find in saliva?
Dr. Tom Nabors:
Most of what we learned about saliva was the four basic compounds: water, enzymes, immunoproteins and minerals. Functions of saliva include lubrication, antimicrobial effects, and aids in swallowing, buffering and the beginning of digestion.
Whole Saliva also contains critical microbiological information—especially pathogens that cause dysbiosis and dysfunctional systemic inflammation.
So, first, we want to know if specific pathogenic profiles are present and how many are there.
Paula:
Tom, you mentioned the word “dysbiosis”; what, exactly, does that mean?
Dr. Tom Nabors:
Dysbiosis is a term that simply means that there is an imbalance between the types of microorganisms present in a person’s microflora. When dysbiosis occurs in the gut, this contributes to many inflammatory diseases, including RA, atherosclerosis, ulcerative colitis, Crohn’s disease and both types of diabetes.
Dysbiosis in the mouth is a serious disruption of the normal microflora and normal functions. This leads to dental caries, periodontal disease, alveolar bone loss and tonsillitis.
Relative to the systemic repercussions, a healthy oral microflora is charged with the function of breaking down foods into usable forms of energy. Nitric oxide (NO) is an important example. This is an essential element in both cardiometabolic function as well as cognitive function.
However, when the oral microbiome becomes infected (dysbiosis) with specific pathogens, the production of NO is stopped.
So, oral dysbiosis causes oral infections, teeth infections, and the reduction in essential nitric oxide production.
Steve:
What causes oral dysbiosis?
Dr. Tom Nabors:
We have learned that poor oral hygiene, dietary habits, smoking, inflammation, genetics and systemic diseases are causative of oral dysbiosis. However, we have also learned that very specific pathogenic species are causative in this total picture. And we know that the oral microflora begins very early in childhood and is highly related to the oral flora of the parents and siblings.
A saliva test at any age can detect a dysbiotic oral microbiome by detecting specific oral pathogens that are the results of these causative concepts.
The good news, however, is that a trained clinician can reverse this pattern and restore normal microbiome function, thus improving both oral and cardiovascular health.
(Beyond that, the travel of specific oral pathogens from the mouth throughout the entire circulatory system is especially dangerous to all forms of systemic inflammation and diseases)
Paula:
You mentioned “targets of therapy.” Can you explain?
Dr. Tom Nabors:
We are testing saliva to find the real “targets of diagnosis and therapy” and they are called Keystone Pathogens. These include Aa, Pg, Tf and Td. In our lab, we refer to these four as “high-risk” pathogens.
These four pathogens, when found in sufficient numbers, control the entire oral flora including the subgingival biofilm. While the oral community will contain hundreds of different species, current literature supports these four as the most important keys to dysbiosis and their influence on the entire oral environment through genetic cross talk.
Our saliva test thus changes our targets of therapy from a generalized concept to a personalized one. The test report will provide this information. And our training team can answer more specifically any questions.
Steve:
But aren’t these specific bacteria species only found in really deep pockets?
Dr. Tom Nabors:
No. While this was traditionally taught, recent scientific evidence, as well as our findings in gingivitis cases, is that these high-risk pathogens are also found in seemingly low-risk patients.
Since these pathogens are found in gingival crevicular fluid, on the tongue, and in 1-2 mm crevicular spaces even when there is no bone loss, we can detect them in saliva. And they are predictors of advanced disease regardless of pocket depth if found around teeth or peri-implantitis.
So, whole saliva becomes the “collection medium” that contains microbes from every niche and crevice. Thus, it doesn’t matter how shallow or how deep the pockets are, our technology will find them.
Steve:
So, getting to the profitability point: Does saliva testing improve the practice?
Dr. Tom Nabors:
A simple answer is yes.
But the primary goal for using salivary testing is not about selling tests or selling treatment. The test is a unique window into information unobtainable by any other method.
Thus, don’t think of the test as a source of profit: Instead, think of the test as the means to an end. The bigger picture means moving patients into comprehensive therapy vs. less comprehensive therapy because of the test. The test itself should be included in your examination of all patients.
What we found along this journey—and what every practice will find—is that when we develop the skills to understand these tests, that our focus changes, our conversations change, our treatment success improves, our referrals grow, and we see patients ask for treatment rather than ask to defer treatment.
Thus, the practice will see a rapid growth in profitability as a result of doing the right thing for the right reasons.
So, while profit isn’t our primary goal, it becomes an important residual effect.
And the process is quick and simple. The saliva kits provide everything needed for collecting 1ml of whole saliva from the patient. This sample is sent to a clinical laboratory that can analyze the ingredients using DNA technology. Once it’s analyzed, an easy-to-read report is sent within two days through a secure portal to your office.
Paula:
What is the benefit for the patient?
Dr. Tom Nabors:
Our patients want to be healthy. And a saliva test provides information about both their oral health as well as their overall health. These test results speak for themselves just as a blood serum report would speak for itself. Thus, the test report actually becomes the “authority” on disease and the clinician allows the report to encourage the patient to make the right decision. There is no selling in this model. The test report sells itself. Our lab has hundreds of scientific reviews that are available on these links and associations.
Paula:
What is the benefit for the clinician?
Dr. Tom Nabors:
The laboratory report becomes the diagnosis: not the periodontal probe, not bleeding, not pocket depth, and not staging and grading. While this information is helpful, none of the above is a diagnosis.
Up until this type of DNA technology, we didn’t know about the role of a healthy microbiome and its effect on cardiovascular disease. And we were guessing at disease causation and talking about “pockets’ and “bleeding,” which are symptoms of disease, not causative events. Plus, we were guessing at disease resolution after treatment.
We have been using the wrong “diagnosis” system and a model of treatment that isn’t personalized to the disease. Our patients leave with a traditional prophy, or a traditional SRP, and they are still infected. Thus, they reinfect themselves as well as their other family members.
With a saliva test before treatment and approximately 30 days post treatment, we can know how successful our treatment is and how successful our home care regimen is. So, we say … “Stop Guessing” and “Treat the Cause … Not the Symptoms.”
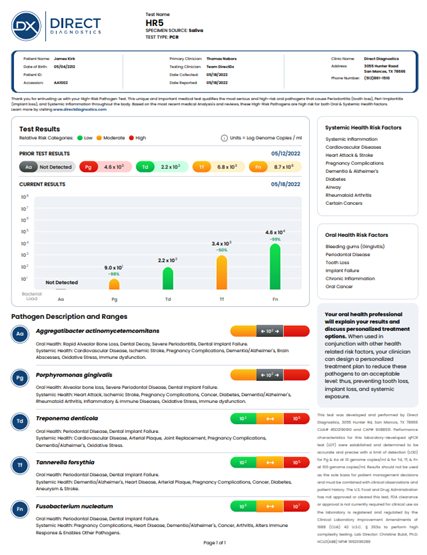
Click below to view this sample diagnostic report:
Now let’s review…
Our profession needs to change quickly to this model. Periodontology is way behind everything else in dentistry. Yes, we have lasers, trays, antibiotics, holistic products, probiotics and other treatment/maintenance products. And I sincerely love this movement to a holistic approach to periodontology.
However, we must be able to predict disease, prevent disease and personalize treatment of disease. We are doing none of these three at a scientific level without a saliva test.
Saliva testing benefits the practice by providing a medical diagnosis and a medical reason to move patients into comprehensive periodontal therapy vs. prophies (“watching and waiting”).
Obviously, periodontal treatment, when presented for the right reasons and conditions, in comparison to 6-month prophies, increases revenue and profitability. Many practices grow 2 – 3 times revenue within the first year when fully adopting saliva testing. And, as time goes by, some offices are seeing that the revenue from their periodontal department (aka hygiene department) can become as large as the entire restorative department. I prefer to call this part of the dental practice “The Disease Prevention Center.”
I can’t overemphasize this point: When the whole team learns how they are stopping this circle of reinfection and in improving overall health, it changes the energy, the focus, and the self-satisfaction of the hygiene team, and the entire office team, with all of us directed toward improving our patients’ overall health.
Steve:
How do I start with saliva testing?
Dr. Tom Nabors:
Find a laboratory with the most experience in clinical application, in the latest technology, and find one that has a complete educational model and clinical support. Our lab is unique because we have the longest number of years in clinical application by our educators and trainers. Plus, we have an entire community of like-minded practices in both dentistry and medicine that will help support new practices.
Paula:
What is the cost of a single test?
Dr. Tom Nabors:
At our lab, the cost is $68. However, for those practices that test often, that cost can be reduced to $57 per test.
Paula:
Does the AAP recognize saliva testing?
Dr. Tom Nabors:
Yes, both the American Academy of Periodontology and the European Federation of Periodontology recognize the value of saliva testing. However, while we have periodontists who use our test, not every periodontist is educated on this important new technology.
Steve:
Tom, thank you for this informative conversation. Do you have any concluding remarks?
Dr. Tom Nabors:
Thank you, Steve and Paula, for asking me to share this information. My final thought is this …
Saliva testing has already become a most important test in preventive medicine. Because we have this technology, we are partnering with medical offices around the country, and they are looking for dental practices to partner with.
The dental practice will become the most important preventive healthcare model within medicine. So, we must prepare ourselves and our practices for this transition and for our collaboration with other physicians.
